 Newman Regional Health team members (L to R) Cathy Pimple, Chief Quality and Compliance Officer; Nina Topper, Clinical Analyst; Dr. Alana Longwell, Hospitalist and Inpatient Rehabilitation Medical Director; and Aubrey Arnold, Care Manager.
Newman Regional Health team members (L to R) Cathy Pimple, Chief Quality and Compliance Officer; Nina Topper, Clinical Analyst; Dr. Alana Longwell, Hospitalist and Inpatient Rehabilitation Medical Director; and Aubrey Arnold, Care Manager.
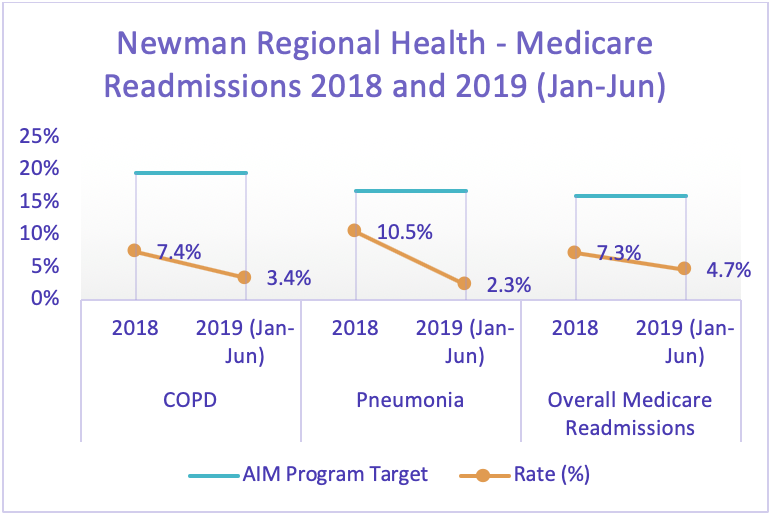
Although readmission rates were already lower than their target, leadership at Newman Regional Health thought they could further reduce them.
Cathy Pimple is Chief Quality and Compliance Officer at the not-for-profit 25-bed critical access hospital in Emporia, owned by the citizens of Lyon County, Kansas. She said they recognized that those at highest risk for readmission in their community shared something in common.
“We recognized that our high-risk patients were individuals who had multiple chronic illnesses,” Pimple said. “So, in order to better address their needs, we developed an Advanced Illness Management (AIM) program, which was aimed at improving care transitions.”
Newman Regional Health’s AIM program consists of four basic steps:
- Identify high-risk patients;
- Before discharge, consult with those identified about benefits of program;
- After discharge, visit enrollees in the program at home to assist with medication self-management, follow-up with primary care provider, communicate the red flags of their conditions and when contact the provider, and establish connection to community resources; and
- Follow-up calls for 30 days up to six months.
“Obviously we didn’t create this model of care,” Pimple said. “Rather we took components of it from projects and programs that we learned about. We took from those successes in the literature and we re-engineered them to make it work for our small rural hospital.”
Newman Regional Health is among the nearly 180 clinics and hospitalist programs across the state that are part of the Kansas Practice Transformation Network, or PTN. It is also part of another core KHC initiative, the Hospital Improvement Innovation Network, or HIIN.
Clinics participating in the PTN receive in-person assistance from the Kansas Healthcare Collaborative as they work on initiatives to improve health care quality and patient safety. KHC Quality Improvement Advisors tailor their technical assistance to each practice’s needs, including transitions of care, preventative care, chronic condition management, and cost reduction and savings.
 Early promise of AIM
Early promise of AIM
When the Newman Regional Health team crafted AIM in 2016, the hospital’s Medicare 30-day readmission rate was between 12-14%. In the last year, 100% of the patients enrolled in the AIM program (about 80) had no 30-day readmission to the hospital. The hospital’s Overall Medicare Readmissions rate for 2018 was down to 7.3%. The benchmark for Medicare 30-day readmission rate is 16%.
Pimple attributes the program’s early success to her team members’ unique strengths—starting with the bedside conversations with high-risk patients before they leave the hospital. She suspects Newman Regional Health is able to enroll a much higher percentage of patients identified as high-risk thanks to Care Manager Aubrey Arnold.
“One of the things Aubrey does exceptionally well is connect with people,” Pimple said. “She forms that relationship with patients, and I think that means more of them are receptive to the program. That certainly affects the outcomes that we have with the program.”
“I’ve read that for transition programs out of hospitals, it’s not uncommon for about half of patients to decline the services after they are offered.” Pimple said Newman Regional Health’s enrollment rate has been closer to 75%.
The bed-side conversation
Aubrey Arnold said she has studied health coaching and credits those techniques for helping in the bed-side conversations.
“I go into their hospital room and we discuss the different things we can offer them in the program,” Arnold said.
“A lot of the conversations revolve around medication management, understanding the disease process, and educating them on different things like—if they are a heart-failure patient—taking daily weights and watching their sodium intake,” she said.
“In that conversation, I try to identify their needs, so that then when I go to their house I can follow up on those needs. For example, I find out whether they are in need of community resources, perhaps a social worker's help in applying for Medicaid, and address care coordination.”
The critical role of data
Pimple also attributed the program’s early success to Clinical Analyst Nina Topper.
“This program depends on data, so Nina's role is critical,” Pimple said. “She extracts all the readmissions for us. For those patients who did not enroll in the AIM program, but we had a readmission, it’s helpful for us to understand: Did we follow the best practice? Or was there a deviation? Was it a preventable readmission?”
“That's a critical component. If we didn't have Nina digging in the charts and getting us the information we need to provide that performance improvement, we wouldn't be able to continually improve the program and we wouldn’t be where we are today,” she said.
For example, in 2018 the team decided to make two significant changes in the program that Pimple says have been a success. First, they doubled the staff time allotted to the program from a half-time to a full-time employee—allowing them to enroll more patients in the program.
Second, they implemented a more rigorous way of identifying patients at high risk for readmission. Originally, they flagged patients who had been admitted to the hospital within the last 30 days.
“After re-evaluating, we incorporated L.A.C.E. scoring to fortify our identification of patients for the program,” Pimple said.
The scoring method rates patients on four risk factors: Length of stay, Acuity of admission, Co-morbidities, and ER visits in the last six months. Patients who score higher than 10 are at high risk of readmission within 30 days.
Pimple said they don’t enroll 100% of patients who score higher than 10. “What the L.A.C.E. test does is to trigger the conversation by Aubrey at the interdisciplinary meeting about modifiable behaviors that she can work with them on in the community setting to keep them healthy and from needing to come back in.”
Continually working to improve
The Newman Regional Health team is proud of the AIM program’s early success, Pimple said, and it’s helped spur other improvement efforts.
The hospital is currently beginning a chronic care management program and is working with the first 10 patients enrolled in the program.
“We are already starting to see improved patient experience through the program, anecdotally. So, we're super excited about that—and I expect through this program we’re going to reach a much larger population than we have through the AIM program.”
The KHC Quality Improvement Advisor who works with Newman Regional Health is Patty Thomsen. Her work with the program led to a $20,000 KHC Quality in Action grant to help launch the chronic care management program. Now she is helping ensure that the team is prepared for the next phase in quality improvement from the Centers for Medicare & Medicaid Services: the Clinician Quality Improvement Contractor, or CQIC.
“Newman Regional Health’s quality improvement work will continue to be an evolving story,” Thomsen said. “When you look at the aims for the upcoming CQIC initiative, it just perfectly lines up for Newman Regional Health and for their programs to continue to evolve.”